Heart failure with Atrial fibrillation in Elderly female
60 years old female Patient presented to casualty with symptoms of palpitations and increasing severity of shortness of breath
Pedal edema ,dry cough .
On examination:PRIMARY SURVEY
patient is tachypneic-RR-36/min
Afebrile,profusely sweating
Raised Jugular venous pressure
Bilateral grade 2 pitting edema
Pulse Rate - 150 beats / min,Irregular
BP- 130/80 mmhg
Spo2-94% at room air

Video showing raised jugular venous pressure
Respiratory system - decreased breath sounds heard over left inframammary,infraxillary,infrascapular region
Cardiovascular system - s1 and s2 heard
immediately ECG was done that showed narrow complex tachycardia with irregular rhythm with absent P waves Suggestive of Atrial Fibrillation
Patient was shifted to ICU
And was given Inj. Amiodarone Stat And infusion continued for 24 hrs along with other supportive treatment . Patient heart rate decreased to 120/min and continuous ECG monitoring was done .
After patient got stabilised detailed history was taken;
Patient gives history of
1. Shortness of breath since 10 days ,that gradually progressed from grade 2 to grade 4, there is history of orthopnea ,PND .
2. Dry cough since 10 days ,increasing on lying down ,patient is comfortable on lying on left side ,no cold,
3. Palpitations since 10 days that gradually progressed .
4.sudden onset of bilateral Pedal edema since 10 days, that initially started in foot and extended till knee
H/o palpitations 40 years back
No h/o chest pain,chest tightness
No h/o seasonal variation Of cough,shortness of breath
No h/o wheeze
No h/o weight loss
PAST HISTORY ;
30 years back patient developed bilateral lower leg weakness following LSCS ,during her last child birth ,and walked with support for 6 months
3 years back following her brother demise patient was emotionally disturbed and noticed involuntary blinking of left eye and deviation of mouth to left side ,then in year of 2019 CT IMAGING was done that showed Acute Infarct in left inferior and middle cerebellum
9 months back patient had underwent right D-J stenting
No history of Diabtes , Hypertension ,Asthma,Epilepsy ,Coronay Artery Disease .
Provisional Diagnosis :
Heart Failure with Atrial fibrillation
K/c/o Cerebrovascular accident
Patient was investigated further :

ECG-showed irregular heart rate with absent P waves ,serial ECG show irregular heart rate -narrow complex tachycardia

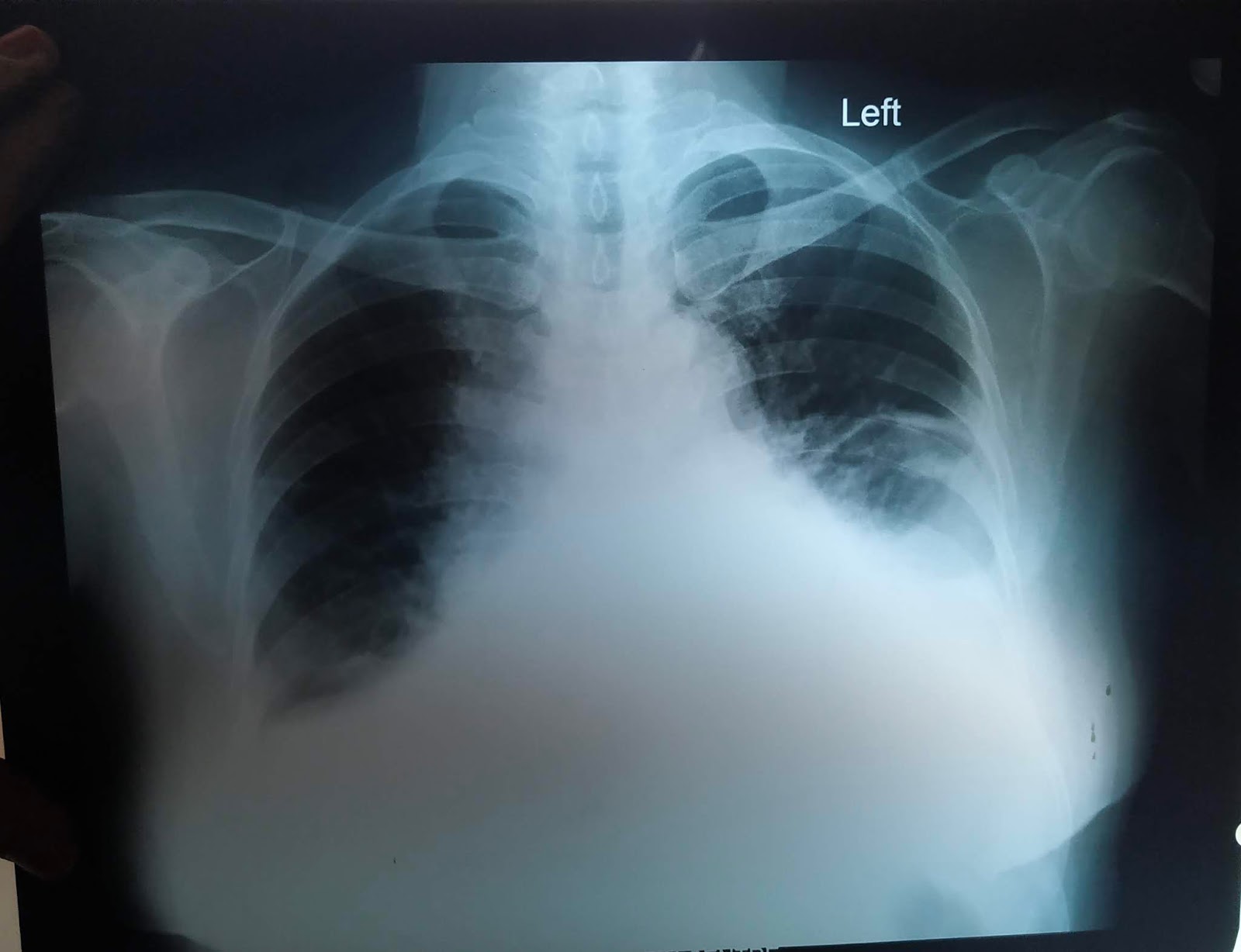
Chest x ray - showed obliteration of both costochondral angle suggestive of Bilateral pleural effusion

Pleural tap was done on day 2 of Admission that showed transudative pleural effusion

2D Echo revealed : Dilated left Atrium and Ventricle
With reduced ejection fraction- 30 % {visual ejection fraction }
Other investigations showed
Serum protein -5.2
Final diagnosis ;
Heart failure with reduced ejection fraction
Atrial fibrillation Secondary to heart failure
Bilateral pleural effusion due to heart failure
Pedal edema ,dry cough .
On examination:PRIMARY SURVEY
patient is tachypneic-RR-36/min
Afebrile,profusely sweating
Raised Jugular venous pressure
Bilateral grade 2 pitting edema
Pulse Rate - 150 beats / min,Irregular
BP- 130/80 mmhg
Spo2-94% at room air

Respiratory system - decreased breath sounds heard over left inframammary,infraxillary,infrascapular region
Cardiovascular system - s1 and s2 heard
immediately ECG was done that showed narrow complex tachycardia with irregular rhythm with absent P waves Suggestive of Atrial Fibrillation
Patient was shifted to ICU
And was given Inj. Amiodarone Stat And infusion continued for 24 hrs along with other supportive treatment . Patient heart rate decreased to 120/min and continuous ECG monitoring was done .
After patient got stabilised detailed history was taken;
Patient gives history of
1. Shortness of breath since 10 days ,that gradually progressed from grade 2 to grade 4, there is history of orthopnea ,PND .
2. Dry cough since 10 days ,increasing on lying down ,patient is comfortable on lying on left side ,no cold,
3. Palpitations since 10 days that gradually progressed .
4.sudden onset of bilateral Pedal edema since 10 days, that initially started in foot and extended till knee
H/o palpitations 40 years back
No h/o chest pain,chest tightness
No h/o seasonal variation Of cough,shortness of breath
No h/o wheeze
No h/o weight loss
PAST HISTORY ;
30 years back patient developed bilateral lower leg weakness following LSCS ,during her last child birth ,and walked with support for 6 months
3 years back following her brother demise patient was emotionally disturbed and noticed involuntary blinking of left eye and deviation of mouth to left side ,then in year of 2019 CT IMAGING was done that showed Acute Infarct in left inferior and middle cerebellum
9 months back patient had underwent right D-J stenting
No history of Diabtes , Hypertension ,Asthma,Epilepsy ,Coronay Artery Disease .
Provisional Diagnosis :
Heart Failure with Atrial fibrillation
K/c/o Cerebrovascular accident
Patient was investigated further :


 |
| After 3 days of treatment ecg showed regular rhythm with tachycardia |
Chest x ray - showed obliteration of both costochondral angle suggestive of Bilateral pleural effusion
Pleural tap was done on day 2 of Admission that showed transudative pleural effusion

2D Echo revealed : Dilated left Atrium and Ventricle
With reduced ejection fraction- 30 % {visual ejection fraction }
Other investigations showed
Serum protein -5.2
Final diagnosis ;
Heart failure with reduced ejection fraction
Atrial fibrillation Secondary to heart failure
Bilateral pleural effusion due to heart failure


Comments
Post a Comment